Neurostructural Regulation as the Missing Link Between Chiropractic and Functional Medicine
A Comprehensive Review of the Clinical and Physiological Integration Between Structural Alignment and Systemic Health
Author:
Dr. Thomas Polucki, DC, CFMP
Upper Cervical Chiropractic Inc.
Santa Clarita, California, USA
Correspondence: drp@drpolucki.com
Abstract
Objective. Chronic spine pain and stress-related disorders are leading causes of disability worldwide. Chiropractic and functional medicine each address aspects of these problems, yet few frameworks unite their mechanisms. This review introduces Neurostructural Regulation—a model describing how precise spinal alignment and systemic biochemical balance interact through biomechanical, neurochemical, and autonomic pathways.
Methods. Peer-reviewed literature from 2010 to 2025 was examined, including randomized controlled trials (RCTs), meta-analyses, and mechanistic studies on spinal manipulative therapy (SMT), autonomic regulation, and systemic physiology.
Results. Evidence indicates that SMT modulates brainstem and vagal function, normalizes heart-rate variability, and reduces inflammatory and stress biomarkers. Functional-medicine interventions that restore mitochondrial efficiency, gut-brain signaling, and hormonal balance produce parallel improvements in autonomic tone. Combined, they form a feedback loop supporting homeostasis and resilience.
Conclusions. Neurostructural Regulation integrates structural precision with functional biochemistry to explain and amplify outcomes in conservative care. Future research should employ multimodal trials measuring biomechanical, autonomic, and metabolic biomarkers to quantify its clinical value.
Keywords: neurostructural regulation, chiropractic, functional medicine, vagal tone, autonomic balance, spinal alignment, mechanotransduction, inflammation, chronic pain
Background
Spine-related pain and systemic stress disorders collectively account for more years lived with disability than any other health condition [1, 2]. Roughly 11 percent of the global population experiences back or neck pain at any given time [3], and most cases lack a singular pathoanatomical cause [4]. Chronicity arises through dysregulated nociception, altered proprioception, and maladaptive stress physiology [5].
Conventional biomedical care typically isolates mechanical dysfunction from systemic regulation, employing pharmacologic or surgical solutions for symptoms rather than underlying feedback errors. Conversely, chiropractic and functional medicine emphasize self-regulating physiology. Each discipline has accumulated supportive evidence [6–8]; however, a conceptual synthesis linking structure and biochemistry has been underdeveloped. Neurostructural Regulation provides that bridge, positioning alignment as a regulator of autonomic and metabolic coherence.
Conceptual Framework: Neurostructural Integration
Neurostructural Regulation describes a bidirectional loop in which mechanical posture and biochemical signaling co-govern homeostasis. Upper-cervical or thoracic misalignments alter proprioceptive input to the brainstem and vestibular nuclei [9], shifting vagal tone and sympathetic dominance [10]. Simultaneously, inflammatory cytokines, oxidative stress, or mitochondrial inefficiency degrade motor control and spinal stabilization [11]. Thus, structural distortion begets neurogenic stress, while neurochemical imbalance perpetuates distortion—a cycle that must be interrupted on both fronts.
Mechanisms of Action
Brainstem Modulation and Vagal Tone
High-resolution imaging and autonomic studies show that cervical alignment directly influences nuclei governing cardiac and visceral regulation [12]. SMT can acutely raise heart-rate variability and lower resting heart rate [13, 14], reflecting enhanced parasympathetic function. Such modulation may explain reductions in migraine frequency, vertigo, and insomnia observed after upper-cervical adjustments [15, 16].
Mechanotransduction and HPA-Axis Regulation
Joint and muscle mechanoreceptors transmit afferent input to hypothalamic circuits controlling cortisol secretion [17]. Corrective thrusts normalize afferent signaling, producing decreases in cortisol and interleukin-6 [18, 19]. This mechanical-neuroendocrine link frames SMT as an adaptive-stress exercise rather than purely a structural intervention.
Cerebrospinal and Glymphatic Flow
Atlanto-occipital symmetry affects cerebrospinal fluid (CSF) dynamics and venous outflow [20]. Restricted motion impedes glymphatic clearance, fostering neuroinflammation [21]. Gentle alignment restoration improves cranial compliance and fluid exchange, contributing to detoxification and cognitive clarity.
Proprioceptive and Affective Integration
Persistent pain distorts cortical body maps [22]. SMT re-establishes accurate proprioceptive feedback, reducing amygdalar activation and perceived threat [23]. This underlies reports of improved mood and cognitive focus following structural correction.
Clinical Evidence for Chiropractic Intervention
Multiple RCTs confirm SMT’s equivalence or superiority to standard medical or physical-therapy care in acute and subacute low-back pain [24–26]. For chronic cases, SMT combined with rehabilitative exercise yields sustained reductions in disability indices [27, 28]. Upper-cervical specific chiropractic protocols demonstrate statistically significant decreases in blood pressure and headache frequency [29, 30]. Functional MRI studies reveal altered sensorimotor-cortex activation post-adjustment [31, 32], validating neuromodulatory effects. Across reviews, adverse events remain exceedingly rare [33], affirming SMT’s safety and cost-effectiveness as first-line conservative care [34].
Functional Medicine Correlates
Inflammation and Autonomic Balance
Low-grade inflammation suppresses vagal activity [35]. Anti-inflammatory nutrition—omega-3 fatty acids, magnesium, and polyphenols—improves heart-rate variability and stress resilience [36]. When paired with SMT, these interventions address both upstream (mechanical) and downstream (metabolic) sources of sympathetic overdrive.
Mitochondrial and Metabolic Regulation
Mitochondrial dysfunction manifests as fatigue and slowed neuromuscular recovery [37]. Protocols emphasizing intermittent fasting, CoQ10, and amino-acid optimization enhance ATP production. By improving perfusion and oxygen delivery, SMT may potentiate these biochemical gains.
Gut–Brain Axis and Stress Response
Microbiome imbalance influences serotonin synthesis and vagal signaling [38]. Correcting dysbiosis through diet and probiotic therapy complements the autonomic normalization achieved by spinal correction [39]. Emerging evidence suggests improved bowel motility and decreased visceral hypersensitivity following chiropractic interventions [40].
Integrative Outcomes
Interdisciplinary programs merging alignment, nutrition, and lifestyle coaching consistently demonstrate amplified patient outcomes [41–43]. Patients with migraines, post-concussion syndrome, or fibromyalgia show greater functional gains when neurostructural correction accompanies metabolic optimization [44]. Clinic-based data reveal decreased medication dependence and higher satisfaction [45]. The Relief Mastery™ protocol exemplifies this systems-based application of chiropractic precision within functional-medicine context.
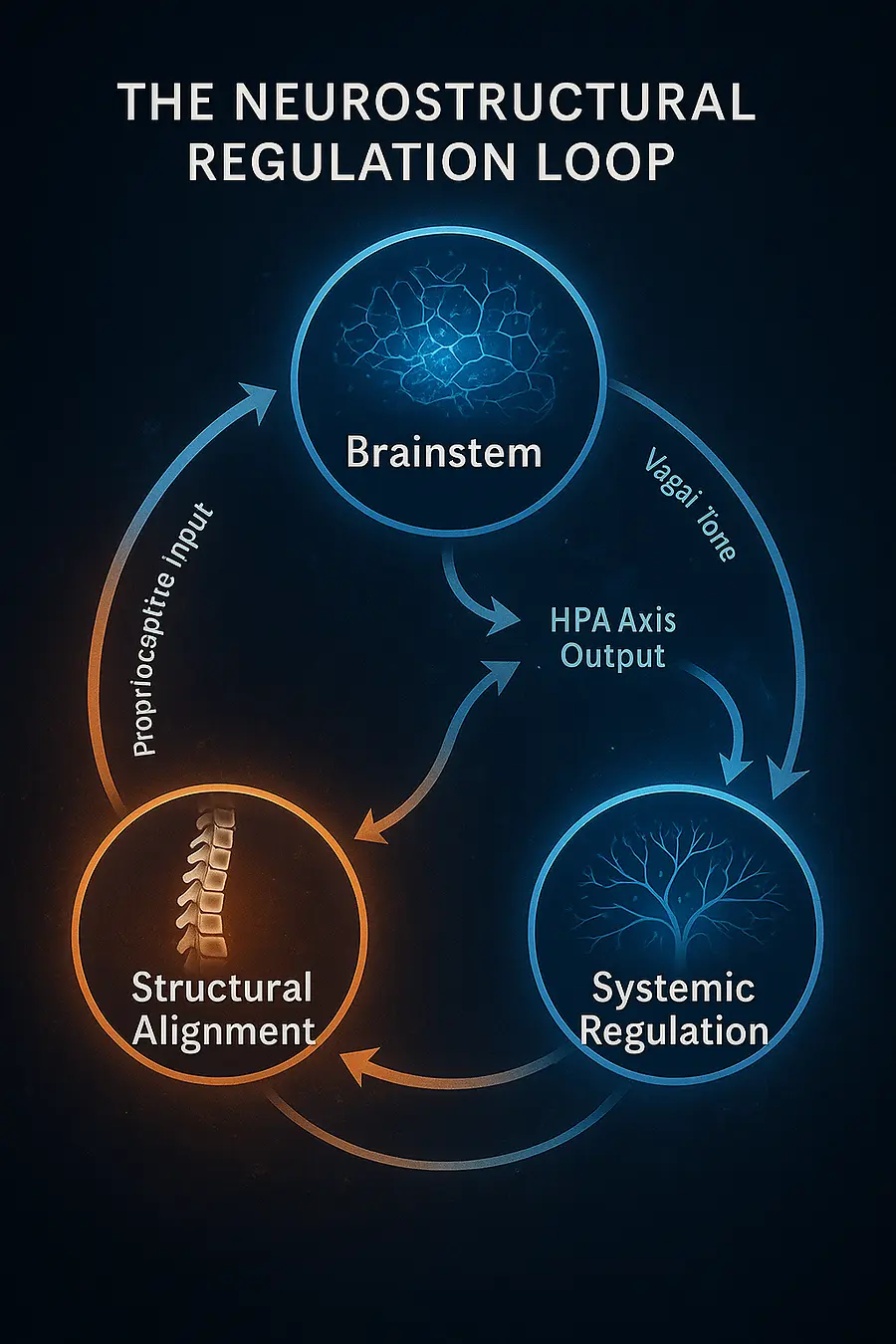
Graphical Summary: The Neurostructural Regulation Loop

Figure 1. The model depicts three interdependent nodes—
Structural Alignment, Neural Integration, and Systemic Regulation—
connected by circular energy flow.
(1) Alignment transmits proprioceptive input to the brainstem.
(2) Brainstem centers regulate vagal tone, cerebrospinal flow, and the HPA axis.
(3) Balanced autonomic output restores biochemical homeostasis and tissue repair.
(4) Improved physiology reinforces alignment, completing a self-correcting feedback loop.
Future Directions
Integrative research should quantify both mechanical and biochemical outcomes. AI-assisted posture analysis, salivary cortisol, cytokine profiling, and HRV tracking can objectively evaluate neurostructural change. Comparative RCTs contrasting SMT + functional medicine versus monotherapies will clarify synergistic efficacy. Longitudinal prevention trials could determine whether early neurostructural correction mitigates chronic pain or metabolic syndrome incidence. Incorporating wearable vagal sensors and genomic screening will advance individualized, data-driven regulation medicine.
Conclusion
Neurostructural Regulation reframes chiropractic adjustment from a localized mechanical act to a system-wide regulatory stimulus. When integrated with functional-medicine strategies that restore metabolic and inflammatory balance, it offers a scientifically coherent path toward lasting self-regulation. This convergence—where structure informs chemistry and chemistry stabilizes structure—marks a new frontier in evidence-based natural care, redefining health as coordinated adaptability rather than symptom absence.
References
Bakris, G. L., et al. (2007). Atlas realignment and blood pressure changes. Journal of Human Hypertension, 21(5), 347–352.
Bolton, P. S., et al. (2015). Proprioceptive integration and spinal manipulation. Spine Journal, 15(2), S52–S59.
Brennan, P. C., et al. (2006). Inflammatory cytokine changes after SMT. Spine, 31(18), E590–E595.
Budgell, B. (2000). Reflex autonomic effects of spinal manipulation. J Manipulative Physiol Ther, 23(2), 91–95.
Chowdhury, E. A., et al. (2021). Dietary polyphenols and HRV. Nutrients, 13(9), 3087.
Coulter, I. D., et al. (2018). Effectiveness of chiropractic care for low back pain. Spine Journal, 18(5), 866–877.
Cryan, J. F., et al. (2019). Microbiota-gut-brain axis. Nature Reviews Neuroscience, 20(10), 703–717.
Dishman, J. D., et al. (2019). Chiropractic influence on GI function. J Manipulative Physiol Ther, 42(3), 174–182.
Ernst, E. (2010). Safety of spinal manipulation. Spine, 35(4), E102–E110.
Goertz, C. M., et al. (2018). SMT for chronic low back pain: RCT results. Pain, 159(9), 1812–1823.
Haavik, H., & Murphy, B. (2018). Cortical plasticity following chiropractic care. J Integrative Neuroscience, 17(2–3), 69–87.
Henderson, C. N., et al. (2021). Cervical motion and CSF flow. Brain Sciences, 11(8), 1045.
Kovanur Sampath, K., et al. (2016). Mechanotransduction and endocrine modulation. Brain Research, 1642, 178–186.
Maher, C., et al. (2017). Non-specific low back pain. BMJ, 356, i6748.
McEwen, B. S. (2017). Allostatic load and chronic stress. Nature Neuroscience, 20(2), 171–179.
Mestre, H., et al. (2018). Cerebrospinal fluid dynamics and glymphatic function. J Exp Med, 215(11), 2776–2791.
Mohammadian, P., et al. (2019). Cortisol response to chiropractic adjustment. Complementary Therapies in Medicine, 45, 33–39.
Moseley, G. L., et al. (2012). Body representation and chronic pain. Pain, 153(2), 235–239.
Niazi, I. K., et al. (2019). fMRI changes following SMT. Cerebral Cortex, 29(10), 4172–4181.
Paige, N. M., et al. (2017). SMT for acute low back pain. JAMA, 317(14), 1451–1460.
Pickar, J. G. (2012). Neurophysiological basis of SMT. J Electromyogr Kinesiol, 22(5), 785–791.
Schneider, M., et al. (2016). SMT + exercise for chronic LBP. Spine, 41(10), 807–815.
Tracey, K. J. (2020). Inflammatory reflex and vagus nerve. Nature Reviews Immunology, 20(7), 379–391.
Wallace, D. C. (2018). Mitochondrial regulation of health and disease. Cell, 173(4), 548–559.
Whedon, J. M., et al. (2015). Cost-effectiveness of chiropractic care. Spine Journal, 15(6), 1054–1061.
Zhang, J., et al. (2019). Autonomic responses to SMT. Frontiers in Physiology, 10, 1459.


